

Is it Safe? AZ overall benefit- risk favourable
Is it Safe? AZ overall benefit- risk favourable
But causal link clearer now

If you find these posts interesting and think others might do so, spread the word.
A short post this week, after both EMA and the MHRA made decisions that the benefits of the AZ vaccine continue to outweigh the risks. In the UK, the JCVI decided out of ‘an abundance of caution’ to advise it was preferable to offer the 20-29 year olds a vaccine other than the AZ vaccine. I wrote a piece at the The Conversation that covers most of this (with links):
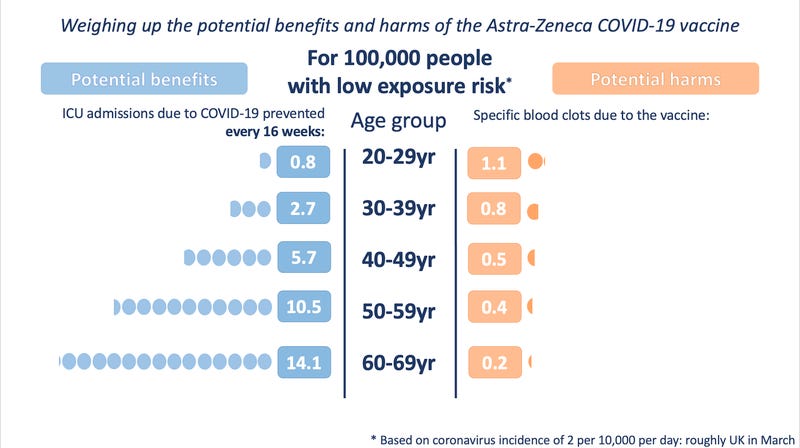
In the UK, the Joint Committee on Vaccines and Immunisation (JCVI) weighed up the risks and benefits of the AstraZeneca vaccine for various age groups. It made an independent recommendation that it would be preferable to offer an alternative vaccine to under-30s, since their risk of severe COVID-19 outcomes, such as intensive care admission, is low when the prevalence of the coronavirus is itself relatively low.
However, as the amount of circulating virus rises, the risk-benefit balance tips in favour of taking the vaccine, regardless of how old you are. If this decision had been made in January, while the second wave was still in full swing, it’s likely that this recommended age restriction wouldn’t have been suggested.
Indeed, presumably in light of this sliding scale of risk, the EMA noted that EU states should now make their own independent decisions about using the vaccine, based on their local COVID-19 status. Many, though, had already introduced quite significant precautionary restrictions on the vaccine while waiting for the EMA’s assessment, limiting its use strictly to older groups.
As I noted in the piece, EU states have further restricted the use of the AZ vaccine., despite having higher levels of COVID-19 in the UK, which would make the risk benefit of the AZ vaccine even more beneficial if the logic of the JVI was used. The Winton Centre for Risk and Evidence Communication created some excellent depictions of risk, which were used in the meeting of the MHRA and JCVI.
I posted some French translations of these to two well known pharmacovigilance experts in France, and I thought this was an interesting response.

Which I think speaks to the cultural difference, and perhaps level of trust in government, that exists in how any further cases might be perceived in France, compared to the UK. In the UK we have explained the risk, and will be warning recipients of the AZ vaccine about the risks. I don’t think an additional case in the UK would become a political issue.
Note, by political I don’t think Prof Moore is suggesting this is politicians seeking to ‘bash the British vaccine’ as some have suggested, but that further deaths in France would be politically difficult to deal with given the state of trust on vaccines in France.
I’ve been impressed by both the MHRA and EMA over the past week, and this short coverage of the briefing in The Guardian seems a fair summary.
When the news is difficult and the science complicated but the desired message is crucial, who better to deliver it than “JVT”, headlining a panel of four top experts in their field?
The government’s choice of Jonathan Van-Tam, England’s deputy chief medical officer, whose metaphors and analogies are legendary, can only have reaffirmed his cult status as the most trusted face of the Covid-19 pandemic in Britain.
The New England Journal of Medicine has a review of 11 cases of Thrombotic Thrombocytopaenia after AZ vaccine, which includes a plausible mechanism. This is discussed in a Science article by Kai Kupferschmidt and Gretchen Vogel, Hard choices emerge as link between AstraZeneca vaccine and rare clotting disorder becomes clearer, in which I comment briefly on causality and on a the potential of reducing risk by reducing the dose (I’m not convinced). They also run through the plausible mechanisms:
Vaxzevria [AZ vaccine] consists of an adenovirus engineered to infect cells and prompt them to produce the virus's spike protein. Among the 50 billion or so virus particles in each dose, some may break apart and release their DNA, Greinacher says. Like heparin, DNA is negatively charged, which would help bind it to PF4, which has a positive charge. The complex might then trigger the production of antibodies, especially when the immune system is already on high alert because of the vaccine. An immune reaction to extracellular DNA is part of an ancient immune defense triggered by severe infection or injury, Greinacher notes, and free DNA itself can signal the body to increase blood coagulation.
Alternatively, the antibodies may already be present in the patients and the vaccine may just boost them. Many healthy people harbor such antibodies against PF4, but they are kept in check by an immune mechanism called peripheral tolerance, says Gowthami Arepally, a hematologist at Duke University School of Medicine who is working as an external consultant with AstraZeneca on the issue. “When you get vaccinated, sometimes the mechanisms of peripheral tolerance get disrupted,” she says. “When that happens, does that unleash any autoimmune syndromes that you are predisposed to, like HIT?”
No doubt this story will rumble on as more information and cases are accumulated, and their may be knock on effects on other adenovirus vector vaccines as EMA has announced they are looking at reports of blood clots in four people who were given the Johnson and Johnson vaccine. The Russian Sputnik V vaccine and CanSino vaccine use similar technology.
Sputnik
There are also concerns about adverse drug reactions associated with the Sputnik V vaccine arising from a whistleblower, and the Sputnik vaccine is being used more as political tool, than it is a vaccine in Russian where only 6% of the population have received it. Plans for countries like Germany to use it without EU approval seem foolhardy. There are also peculiar practices being reported from Slovakia:
Noting that about 40 countries are using or scheduled to use the Russian vaccine, the Slovak regulatory agency asserted that “these vaccines are only associated by the name.” That raised questions about deviations from the formula reviewed in The Lancet.
“The comparability and consistency of different batches produced at different locations has not been demonstrated,” the Slovak regulator said. “In several cases, they appear to be vaccines with different properties (lyophilisate versus solution, single-dose ampoules versus multi-dose vials, different storage conditions, composition and method of manufacture).”
The Slovak statement could damage Russia’s efforts to establish Sputnik V as a reliable brand. It could also exacerbate lingering doubts left by the vaccine’s highly politicized rollout in Russia, where President Vladimir V. Putin announced that the drug was ready for use in August, before clinical trials had finished.
Russia has repeatedly denounced foreign questioning of its vaccine as the fruit of anti-Russian conspiracies and prejudice, ignoring complaints that Mr. Putin, rushing last summer to declare a Russian victory in the race for a vaccine, violated standard procedure by declaring Sputnik V safe before trials had finished.
Never forget
At the bottom of the EMA Press Release this week it was noted that:
'As of 4 April 2021, a total of 169 cases of CVST & 53 cases of splanchnic vein thrombosis were reported to EudraVigilance. Around 34 million people [.] vaccinated in the EEA & UK by this date. The more recent data do not change the PRAC’s recommendations'
Even though tens of thousands of people have died from COVID-19 over the past few months, and in purely utilitarian terms the vaccines are saving more lives than they cost, it should be remembered that every one of these lives is someone’s relative. Every death is a great loss, and all the families concerned will be suffering. The risk balance of a vaccine is at a population level, and as individuals we choose to accept risk at an individual level. Most get the benefits and but some extremely unlucky people get the harms. I was deeply moved by the composure of a fellow pharmacist Alison Astles’ who spoke in favour of vaccination, despite the death of her brother Neil from suspected clot from the AZ vaccine.
That’s all and stay safe.
Anthony
Don’t forget to report your suspected adverse effects from medicines and vaccines. In the UK, this means using the Yellow Card Scheme.
More excellent balanced comment. This blog should be more widely known.