

Is it Safe? Timing is everything
Is it Safe? Timing is everything
STIKO, Lipid nanoparticles, and the BMJ rapid responses.

If you find this post interesting and think others might do so, spread the word.
I was on a panel addressing student concerns about COVID-19 vaccination in our College at the University of Birmingham this past week. We has a great panel of scientists, clinical practitioners, and a local Imam to address concerns. You might think that students on healthcare courses and biomedical don’t have concerns, but they are no different from those already qualified and the general public. The same rumours fly around on WhatsApp and other social media. Merely being on a science degree is not protection against social pressures. But generally, there was a high quality of sensible questions, and it was a useful session.
This tweet comes from Independent SAGE, who should know better.

This is terrible ambiguous framing. Not sure if the ‘Do you feel safe?’ refers to the vaccine safety or if the recipient feels safe from COVID-19.
Independent SAGE is in danger of making an increasing number of missteps as the end game of the COVID-19 pandemic pans out. If they perceive they are becoming insignificant, they may be tempted to make increasingly ‘hot takes’ to gain attention. This will carry reputational risk for those involved, so I am surprised that more aren’t quietly leaving the room now they have had the media attention. I suspect will create an independent SAGE inquiry into the pandemic, and an independent SAGE future pandemic preparedness plan. Oh well.
This article by Hilda Bastian on the ‘100% effective and deaths and hospitalisations’ meme that is common on twitter in The Atlantic is well worth your time.
The data were indeed suggestive of an encouraging idea. Based on the numbers so far, we can expect the vaccines to provide extremely high levels of protection against the most dire outcomes. Still, we don’t know how high—and it’s clear they won’t uniformly cause hospitalizations and deaths from COVID-19 to disappear in vaccinated people.
I think this is important. Too simplistic a message can backfire once you start to get cases of the vaccinated being hospitalised or dying (as is likely given the numbers of people involved). ‘You told us they were 100% effective for death!’ will be the cry, and trust will be the victim.
And you can be vaccine optimist and still think this.
Timing is everything
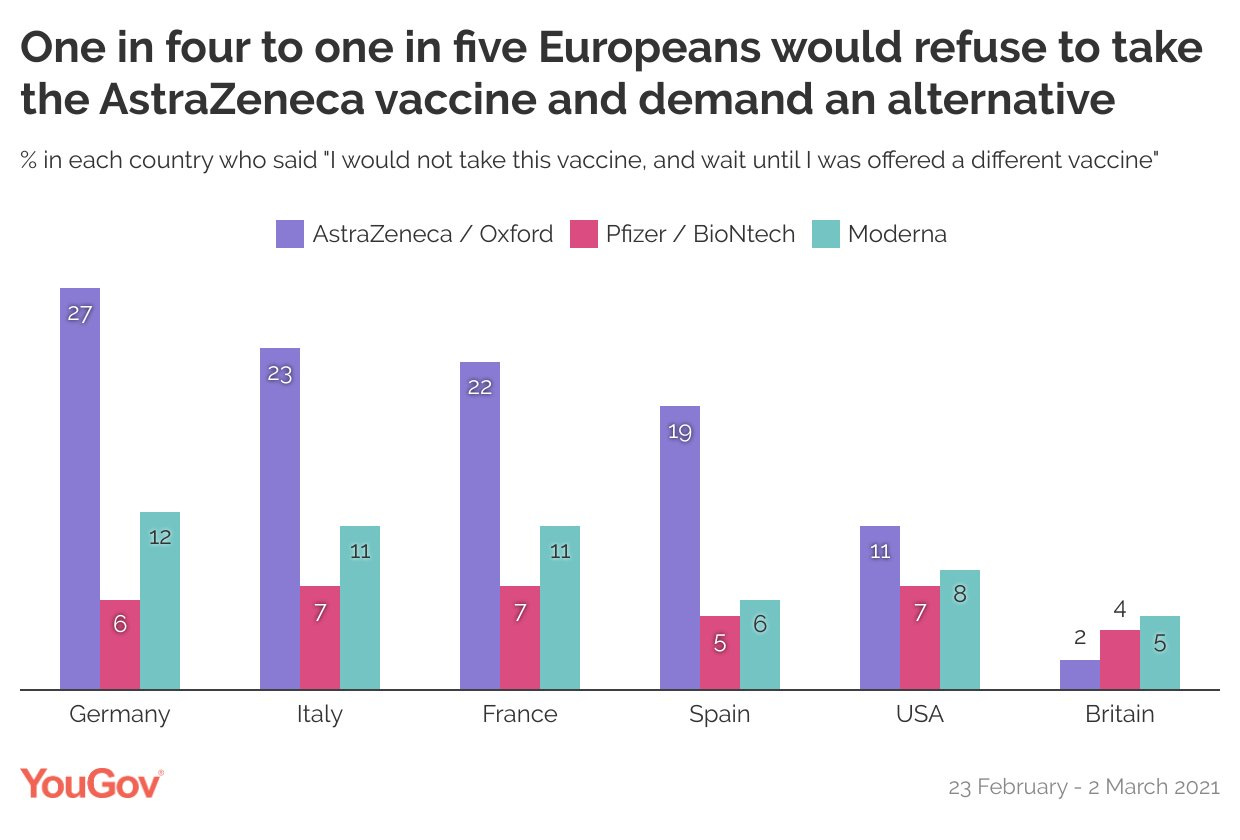
The German Standing Committee on Vaccination (STIKO) has changed its recommendations on the Astra-Zeneca Vaccine. Initially they did not approve its use in the over 65 year old population, but they have now reversed that decision and brought in a 12 week gap for the AZ vaccine (as in the UK). The BBC report on this change, and draws attention to the low uptake and confidence in the AZ vaccine in EU state. A recent YouGov poll highlights this.
It is notable that the European Medicines Agency did licence the AZ vaccine in older patients. This isn’t a story about an EU institution making a mistake. EMA said (my emphasis):
Most of the participants in these studies were between 18 and 55 years old. There are not yet enough results in older participants (over 55 years old) to provide a figure for how well the vaccine will work in this group. However, protection is expected, given that an immune response is seen in this age group and based on experience with other vaccines; as there is reliable information on safety in this population, EMA’s scientific experts considered that the vaccine can be used in older adults.
The German STIKO committee made a different decision than both EMA and the UK’s Joint Committee on Vaccination and Immunisation (JCVI). STIKO appears to have the same make-up as the JCVI, with experts from ‘pediatrics, family medicine, occupational medicine, virology, immunology, epidemiology, public health, and evidence-based medicine.’ It’s not even that they made a ‘wrong’ decision, since there was a lack of data in the older age group.
STIKO seemed to have failed to make an imaginative leap and take the risk of a relatively sure bet based on known science. This has to be placed in the context of a pandemic that is preferentially killing older individuals. Not making the decision the JCVI made has had consequences, both in terms of reducing vaccine supply to the over 65s and in reducing confidence. It would be fascinating to look at the cultures of the JCVI and STIKO in terms of decision making. The JCVI acknowledged the risk of the decision they made, and made it. Possibly brave, but it was a calculated risk that was more than likely to pay off. The STIKO decision was taking a risk with inaction, that on the balance of evidence would be proved wrong. Changing the decision now, after getting confirmatory evidence for the effectiveness in the over 65s, does not give you the same benefit as making the decision the JCVI made weeks ago.
Sometimes a difficult decision made early, is better than an easy decision made later.
It also worth noting that STIKO has brought in the 12 week gap for the AZ vaccine, as in the UK. In the UK there is a certain type of politically partisan activist on social media which has delighted in calling the UK’s delayed dose strategy ‘partial vaccination’, suggesting it was a policy to spin how the UK’s vaccination policy was doing well, rather than a scientific decision that will save lives. Not sure what they think now.
I don’t for one minute think the STIKO decision is the root of all problems with perception of the AZ vaccine in the EU. As soon as it was licenced early in the UK there were German MEPs saying that the regulatory processes in the EU were better than those in the UK, which would have rubbed off on the vaccine, extremely poor media reporting about efficacy in the German Press, and Macron calling it quasi-effective can’t have helped. Clearly the differential trust between the AZ and the other COVID-19 vaccines is about more than the normal cultural differences around vaccination across Europe.
It’s not all about mRNA
The mRNA vaccines are a step change in vaccine technology, but let’s hear a round of applause for the lipid nanoparticles (LNPs) that the fragile mRNA needs to get into your cells and do its magic. They are the unsung heroes of the COVID-19 pandemic and there is years of science behind their development. Chemical and Engineering News has great article on the development of LNPs, and the potential pitfalls, including toxicity.
The vaccines, appropriately celebrated as a first for mRNA technology, are also a milestone for the nanoparticle field. Although the first drug based on an LNP was approved by the US Food and Drug Administration for a rare genetic disease in 2018, the two authorized mRNA vaccines for COVID-19 present a far bigger opportunity for the nanoparticles than even the field’s founders can imagine. “It is a tremendous vindication for everyone working in controlled drug delivery,” says Robert Langer, a chemical engineer at the Massachusetts Institute of Technology.
“LNPs will be going into millions of arms over the course of this year,” says University of British Columbia nanoparticle scientist Pieter Cullis. “What was a fringe field back in the 1980s has turned into something that is mainstream now.”
The BMJ’s Rapid Response system

I tweeted the above this week. As you can see in my tweet, it looks as though the BMJ website has a story titled “Deep concern over vaccination safety”. They don’t. The link is actually to a rapid response to a BMJ article. The BMJ has no concerns about vaccine safety, but the rapid response suggests deaths from the Pfizer and Moderna vaccine “are off the scale” based on reports to the US Vaccine Adverse Events Reporting System (VAERS). This is nonsense. I’m not going to counter it now because of Brandolini's law, but I can assure you that this is utter nonsense.
The rapid response is written by John Stone, the UK editor of Age of Autism. He has a track record of posting material about vaccines on the internet since the turn of the century. He was a frequent commentator at one of the leading UK anti-MMR websites in the 2000s (JABS), and every blogger in the 200s writing about the UK anti-vaccine movement would have come across him.
He uses rapid responses (or those of similarly minded people) as references in posts on other websites. This gives the appearance of BMJ articles supporting his argument, when all they are links to his own arguments or other non peer-reviewed comments. To an uninformed reader, this link looks more impressive that it actually is: https://www.bmj.com/content/372/bmj.n393/rr-4
Rapid responses are relatively easily posted at the BMJ website, and I’m not sure the BMJ should be letting posts about COVID-19 vaccines of this nature be published on their platform, but they definitely should not look like BMJ articles in shortened form on social media.
The Drug Safety Ghost
Did you know there is a ghost, called Lizzie Church, who haunts University College Hospital. She was a trainee nurse in the late 1800s who accidentally overdosed her fiancé on opium, and then killed herself. She apparently hovers over patients receiving morphine today, protecting them from overdose.
That’s all folks. Stay safe.
Anthony
Don’t forget to report your suspected adverse effects from medicines and vaccines. In the UK, this means using the Yellow Card Scheme